Original Research Article
Role of Discharge Summary in Delayed Discharge Process
Roopjot Kochar
Ayurvedic Physician and Nutritionist, 78/13 Anant Nagar, Khanna-141401
ABSTRACT
Delays in the discharge of hospital patients cause a backlog for new admissions from the Emergency Departments, outpatient clinics, and transfers from the Intensive Care Units. A variety of initiatives have been reported on previously which aim to tackle this problem with variable success. While hospital administrators encourage the discharge of patients in the morning to expedite flow through the hospital, often discharges are clustered in the afternoon creating a mismatch between demand and availability of beds in the morning. This mismatch can cause significant overcrowding in the Emergency Department and will affect transfers from Intensive Care Units and elective admissions. The present study has been conducted on 270 patients admitted at a multispecialty hospital of Ludhiana to understand one of major cause of delay in discharge process is delayed preparation of discharge summaries. Turnaround time was recorded from discharge intimation to final summary signed by concerned doctor in order to calculate and study the cause of delay. The present study findings show that majority are taking 3-5 hrs time between discharge intimation and final summary indicating delayed discharge process.
Key words: Discharge Process, Discharge Intimation, Delay in Discharge, Final Summary, Turnaround Time
INTRODUCTION AND REVIEW OF LITERATURE
Delayed discharge or ’bed blocking’ are terms used to describe the inappropriate occupancy of hospital beds. Discharge delays due to lack of availability of post-discharge facilities and waiting for consultant opinions, tests and procedures, have been identified previously. [1] Delayed discharge refers to the situation where a patient is deemed to be medically well enough for discharge but where they are unable to leave hospital because arrangements for continuing care have not been finalized. [2] The problem of delayed discharges in the UK is identified as a system-level issue, leading to inefficiencies in acute bed usage. Discharging patients from the hospital is a complex process that is fraught with challenges and involves over 35 million hospital discharges annually in the United States. Among Medicare patients, almost 20 percent who are discharged from a hospital are readmitted within 30 days, and the cost of unplanned readmissions is 15 to 20 billion dollars annually. [3] Preventing avoidable readmissions has the potential to profoundly improve both the quality of life for patients and the financial wellbeing of health care systems. Discharge planning is the development of an individualized discharge plan for the patient, prior to leaving the hospital, to ensure that patients are discharged at an appropriate time and with provision of adequate post-discharge services. Such planning is a mandatory part of hospital accreditation. [4]
Discharge planning is a complex process that seeks to determine the appropriate level of services required by the patient and then match the patient to an appropriate site of care. [4] This process ideally begins at the start of the hospitalization. The hospital case manager should be involved as soon as it is clear that the patient will require services at home or transfer to an alternative level of care. The decision to discharge a patient from a hospital is a complex process governed by many factors, which comprise not only medical but also organizational reasons, and not all of which are easily controlled. It has been estimated that approximately 30% of hospitalized patients experience a delay of their discharge, while about 30% of these delays are due to non-medical factors. [5]
The primary mode of communication between the hospital care team and aftercare providers is often the discharge summary, raising the importance of successful transmission of this document in a timely fashion. Unfortunately, the discharge summary reaches the primary care provider by the time of the first follow-up visit in only 12 to 34 percent of such visits, and even then often lacks key information. One large, single-center, retrospective study found that a delay in completion of the discharge summary was associated with higher rates of readmission. [6]There was an increase in readmission if the discharge summary was not completed within three days after discharge (odds ratio [OR] 1.09, 95% CI 1.04-1.13) and the risk continued to increase for every additional three days to complete the discharge summary. At the time of discharge, the patient should be provided with a document that includes language and literacy-appropriate instructions and patient education materials to help in successful transition from the hospital. These documents should be brief, focused on critical information to the patient, and primarily directed at what the patient needs to understand to manage his or her condition after discharge. Thus, the present study has been planned to study the role of discharge summary in discharge process.
METHODOLOGY
The present study has been carried out on 270 discharged patients from different wards of different departments to study the discharge process timings in a multispecialty hospital of Ludhiana. Time taken from discharge intimation to final summary by different doctors was recorded to study one of the main causes of delayed discharge process i.e. delay in preparation of final summary.
RESULTS AND DISCUSSION
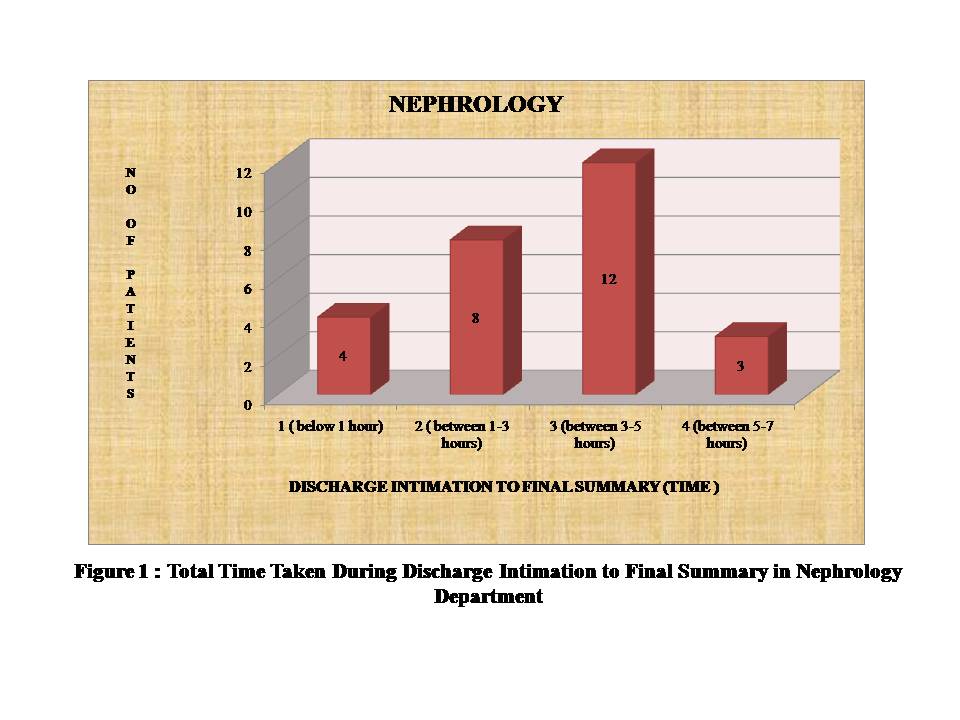
It is shown from figure 1 that in nephrology department discharge intimation to final summary time taken for maximum no. of patients i.e 12 has been observed to be 3-5 hrs followed by 8 patients between 1-3 hrs and for 4 pateints it has been recorded to be below 1 hr while for 3 pateints time taken between discharge intimation to final summary has been found to lie between 5-7 hours.
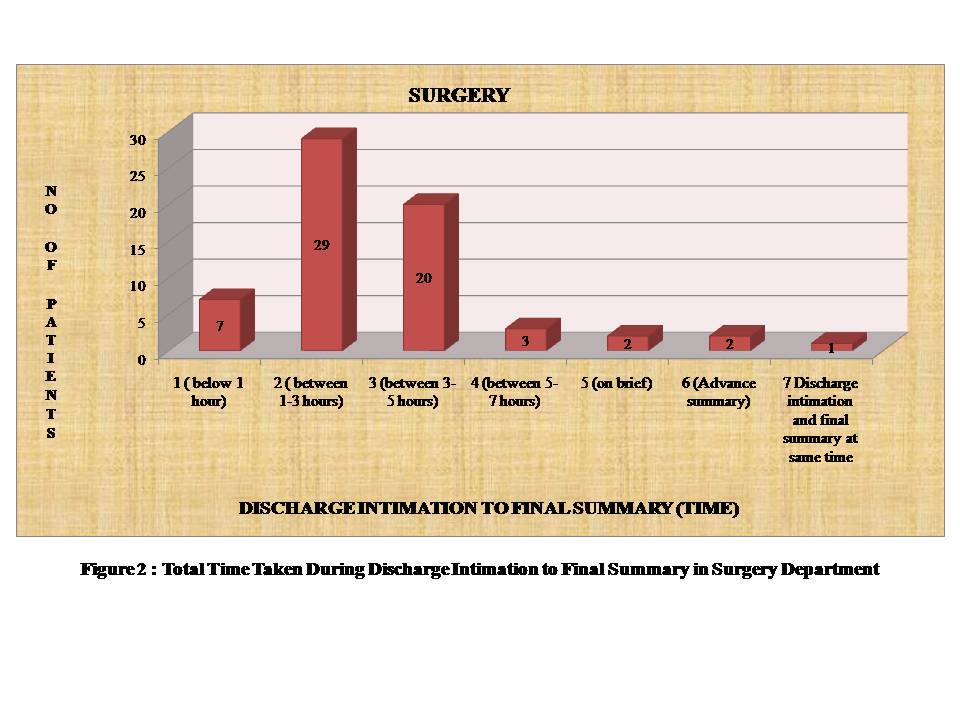
It is observed from figure 2 that in surgery department time taken for maximum no. of patients i.e 29 has been observed between 1-3 hrs for final summary followed by 20 patients between 3-5 hrs and 7 below 1 hr, 2 patients were on brief summary detail and another 2 patients have been on advance summary and 1 patient had no time gap between discharge intimation and final discharge summary.
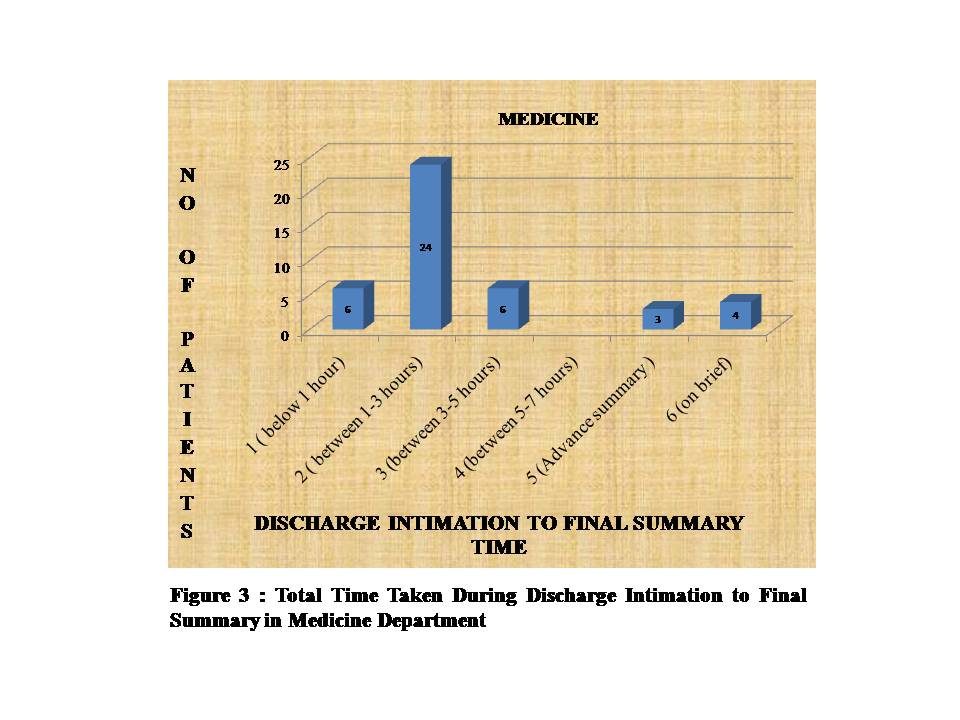
It is observed from figure 3 that time taken for maximum no. of patients (24) is observed between 1-3 hrs for final summary followed by 6 patients each between 3-5 hrs and below 1 hour, 4 pateints were recorded to be on brief summary and 3 on advance summary in medicine department.
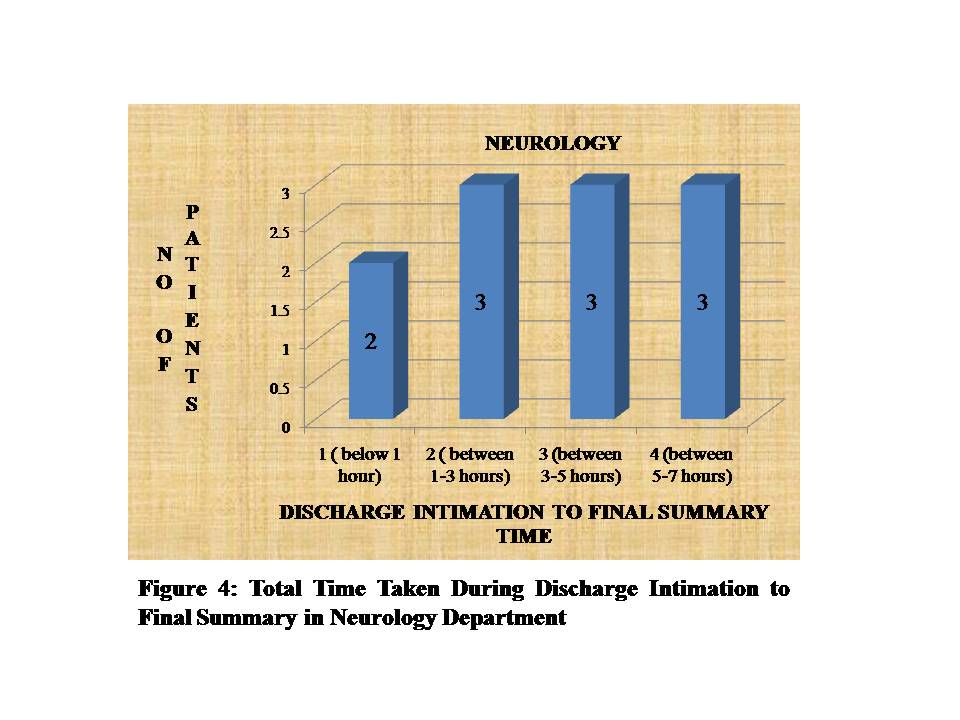
It is observed from figure 4 that in neurology department time taken for maximum no of patients 3-3-3 has been observed between 1-3 hrs, between 3-5 hrs, between 5-7 hrs and for 2 patients it was recorded below 1 hour.
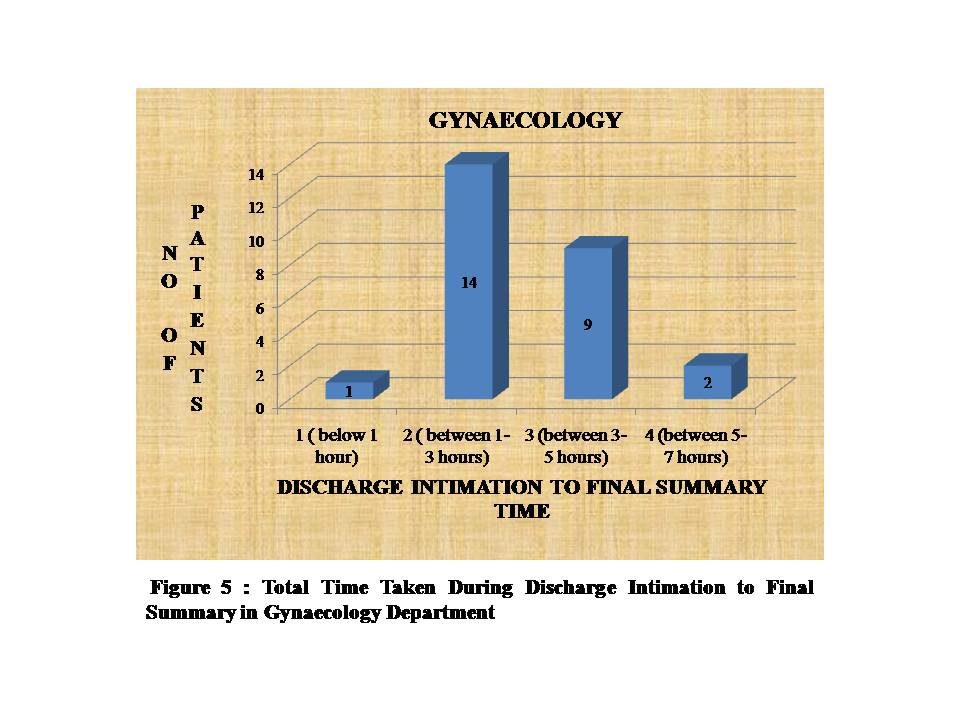
It is observed from figure 5 that time taken for maximum no of patients 14 has been observed to be 1-3 hrs in gynaecology department followed by 9 patients between 3-5 hrs and 2 patients between 5-7 hrs.
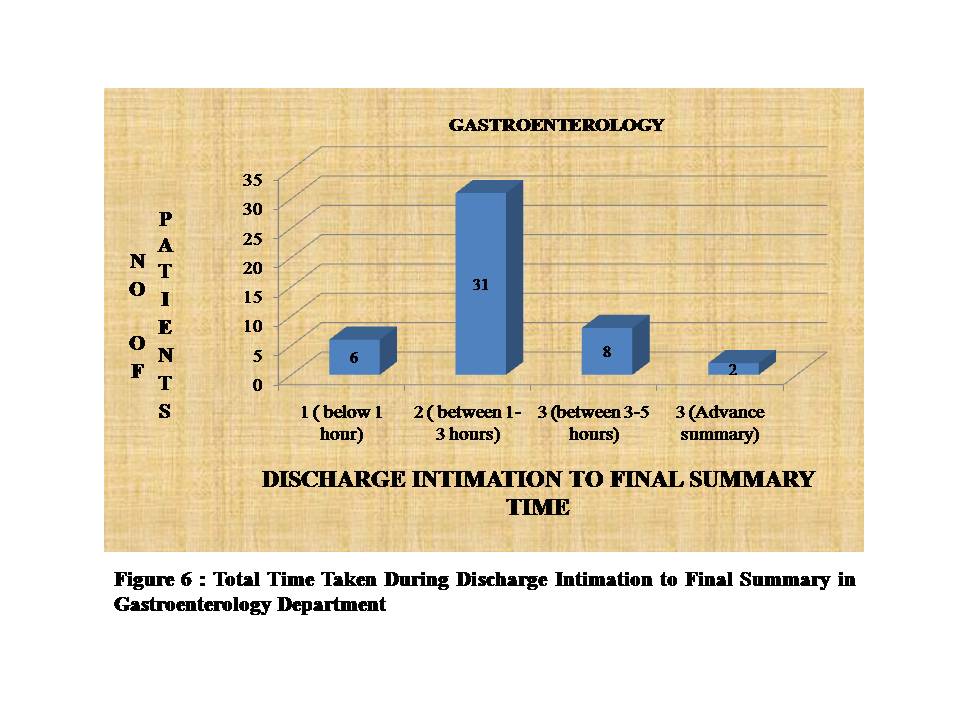
Figure 6 reveals that time taken for maximum no. of patients i.e. 31 has been observed between 1-3 hrs for final summary followed by 8 patient between 3-5 hrs, 6 below 1 hr and 2 pateints were on advance summary in gastroenterology department.
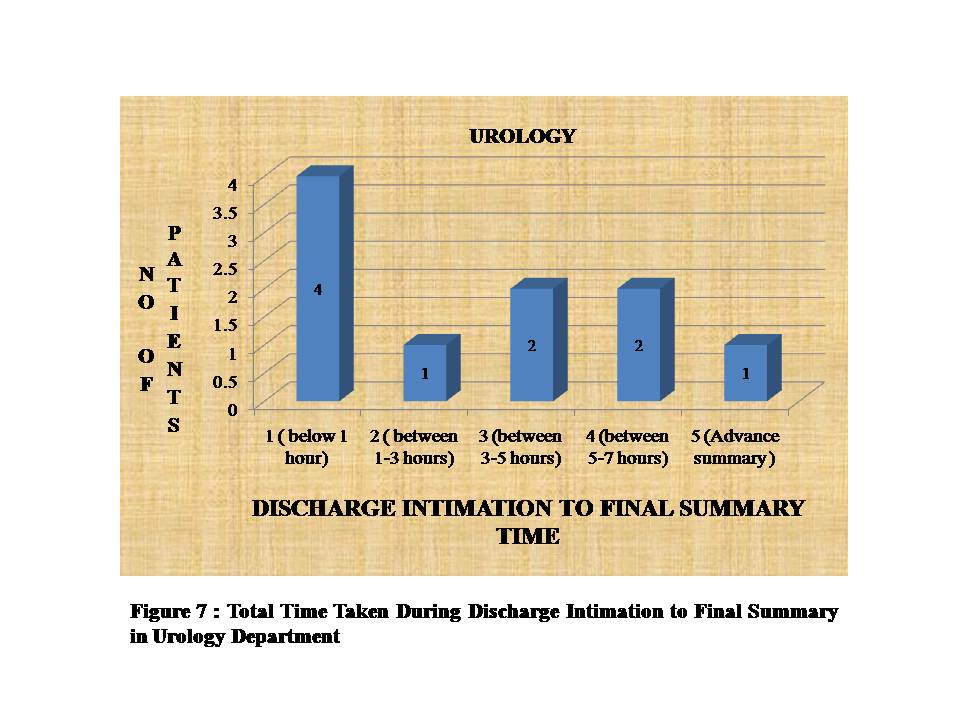
It is observed from figure 7 that time taken for maximum no of patients 4 is observed below 1 hr for final summary followed by 2 -2 patients between 3-5 hrs and 5- 7 hrs, 1-1 between 1-3 hrs and on advance summary resceptively in urology department .
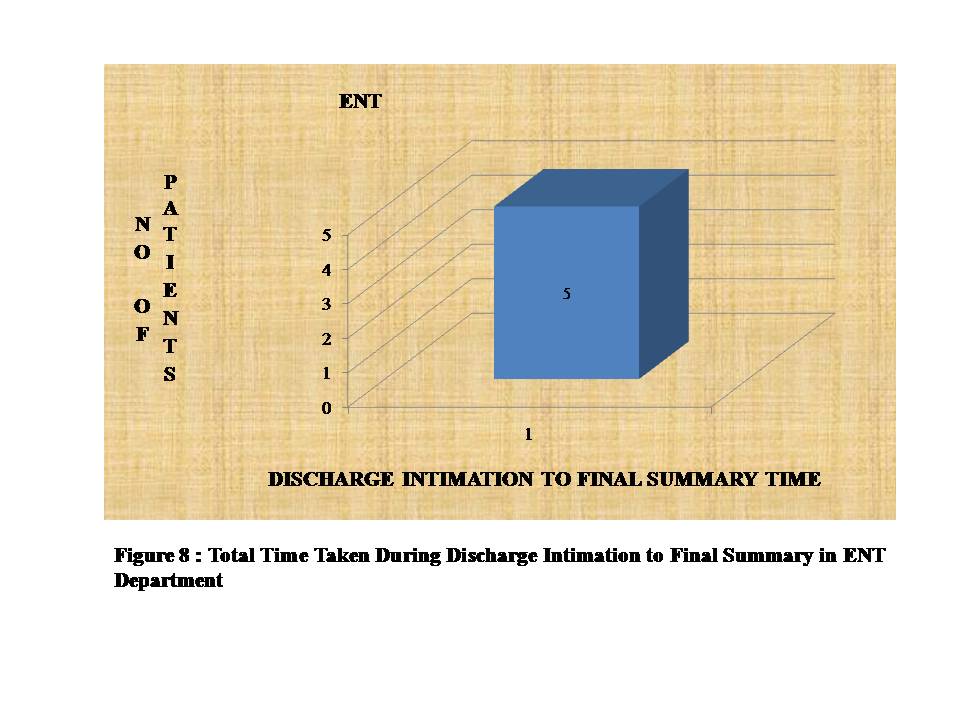
Figure 8 shows that the time taken for maximum no. of patients i.e. 5 in ENT department has been observed between 1-3 hrs for final summary.
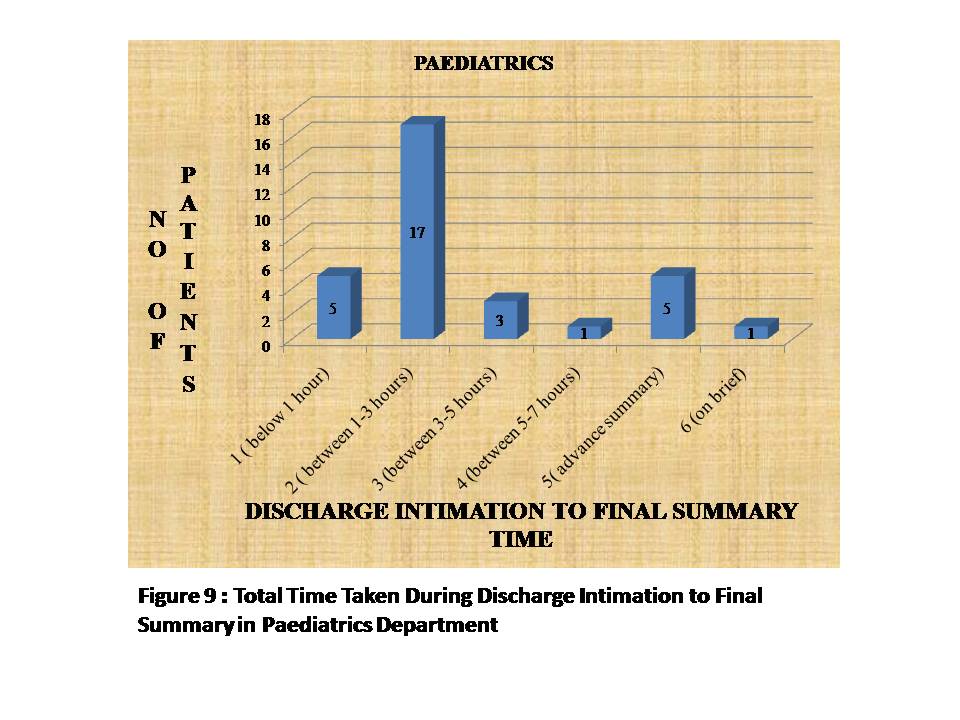
It is observed from figure 9 that time taken for maximum no of patients 17 is observed between 1-3 hrs for final summary followed by 5-5 patients each below 1 hr and on advance summary, 3 patients between 3-5 hrs, 1-1 each between 5-7 hrs and on brief summary respectively in paediatrics department.
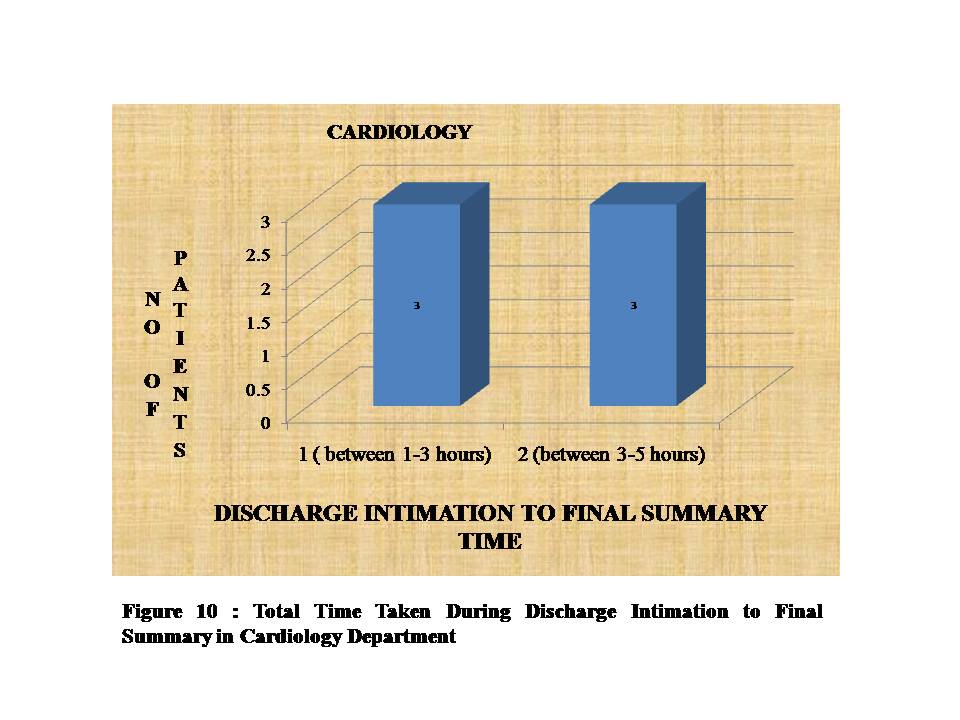
It is observed from figure 10 that time taken for 3 patients has been observed between 1-3 hrs and for another 3 patients it has been recorded as 3-5 hrs in cardiology department.
CONCLUSIONS
Thus, it can be concluded that maximum time i.e. between 5-7 hours has been taken between discharge intimation to final summary in nephrology, neurology, gynecology, pediatrics, urology departments which indicate delay in discharge process. Majority of patients (12) in nephrology department had delayed discharge due to extended discharge intimation to final summary time of 3-5 hrs while good number of patients in other departments including surgery , medicine, gynecology and gastroenterology also had 3-5 hrs of discharge intimation to final summary time indicating it to be one of the major causes of delayed discharge.
REFERENCES
- Muhammad Umair Majeed et al. Delay in discharge and its impact on unnecessary hospital bed occupancy. BMC Health Services Research 2012; 12: 410.
- Karen Bryan; Policies for reducing delayed discharge from hospital. Br Med Bull 2010; 95 (1): 33-46.
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med 2009; 360:1418.
- Shepperd S, McClaran J, Phillips CO, et al. Discharge planning from hospital to home. Cochrane Database Syst Rev 2010; CD000313.
- Ubbink DT, Tump E, Koenders JA, Kleiterp S, Goslings JC, Brölmann FE. Which Reasons Do Doctors, Nurses, and Patients Have for Hospital Discharge? A Mixed-Methods Study. PLoS ONE. 2014; 9(3): e91333.
- Hoyer EH, Odonkor CA, Bhatia SN, et al. Association between days to complete inpatient discharge summaries with all-payer hospital readmissions in Maryland. J Hosp Med 2016; 11:393.
How to cite this article: Kochar R. Role of discharge summary in delayed discharge process. Galore International Journal of Health Sciences & Research. 2016; 1(1): 25-29.